
Metabolic Preservation Strategies: A Clinical Framework for Resistance Training and Nutrient Timing in GLP-1 Therapy
Abstract
The clinical utilization of Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) and dual GLP-1/GIP agonists has fundamentally altered the therapeutic landscape for the management of type 2 diabetes mellitus and chronic obesity. While these pharmacological interventions facilitate significant improvements in glycemic control and induce substantial weight loss, they simultaneously initiate a physiological environment characterized by a rapid and profound caloric deficit. This deficit carries the inherent risk of substantial catabolism of lean body mass (LBM), a consequence that often remains under-addressed in standard clinical protocols. Emerging data derived from large-scale clinical trials and systematic reviews indicate that 20% to 50% of total weight loss during GLP-1 RA therapy may consist of lean mass, with specific cohorts demonstrating muscle loss reaching as high as 60%.1 This erosion of skeletal muscle integrity presents a multifaceted risk profile, contributing to the development of sarcopenic obesity, metabolic rate depression, and a long-term decline in functional independence.
To mitigate these adverse outcomes, this report outlines a comprehensive clinical framework centered on a "Minimum Effective Dose" (MED) resistance training protocol and a targeted nutritional strategy. This framework is designed to satisfy the specific physiological demands of patients on GLP-1 therapy by focusing on the preservation of skeletal muscle, the optimization of mitochondrial function, and the prevention of connective tissue injury. By integrating time-efficient resistance training cadences with precise nutrient timing and amino acid supplementation, clinicians can ensure that the weight loss achieved through pharmacological means is primarily adipose-derived, thereby protecting the patient's basal metabolic rate and reversing biomarkers of cellular aging.
The Catabolic Risk of GLP-1 and Dual-Agonist Therapies
Glucagon-like peptide-1 receptor agonists, such as semaglutide and liraglutide, and dual GLP-1/GIP agonists, such as Tirzepatide, achieve weight reduction primarily through the suppression of appetite and the delay of gastric emptying, which collectively leads to reduced energy intake.4 However, the sustained caloric deficit required for significant weight loss places the human body in a precarious state where the preservation of lean tissue becomes secondary to the utilization of energy stores. Skeletal muscle wasting is a critical determinant of adverse outcomes in metabolic disease, as muscle tissue is not only essential for physical movement but also serves as the body’s largest and most important organ for systemic metabolic health.6
Large-scale clinical trials, including the Semaglutide Treatment Effect in People with Obesity (STEP) and Semaglutide Unabated Sustainability in Treatment of Type 2 Diabetes (SUSTAIN) programs, have highlighted the extent of lean mass loss accompanying semaglutide usage. In a dual-energy X-ray absorptiometry (DEXA) sub-study of the STEP 1 trial, patients receiving 2.4 mg of semaglutide weekly lost approximately 14.9% to 15.0% of their total body weight over 68 weeks.9 While total fat mass and visceral fat mass were significantly reduced, the analysis indicated that lean mass accounted for roughly 39% to 40% of the total weight lost.1 Similar outcomes were observed in the SUSTAIN 8 trial sub-study, where the proportion of weight lost from lean mass reached 43.4%.1 The SURMOUNT-1 trial, which evaluated the dual GLP-1/GIP agonist Tirzepatide, showed a slightly more favorable but still significant lean mass loss of approximately 25% to 26%.1

The implications of these percentages are profound when translated into absolute physiological capacity. Skeletal muscle is responsible for approximately 80% of postprandial glucose uptake under euglycemic-hyperinsulinemic conditions.6 This mechanism is driven by the translocation of the glucose transporter type 4 (GLUT4) protein to the muscle cell membrane, a process that is often impaired in individuals with type 2 diabetes and obesity.6 As muscle mass is depleted during GLP-1 therapy, the surface area and volume available for glucose disposal decrease, potentially exacerbating insulin resistance despite the weight loss. This creates a metabolic paradox where the patient appears "healthier" due to reduced adipose tissue, but remains "metabolically vulnerable" due to a compromised glucose disposal reservoir.1
Furthermore, skeletal muscle serves as the primary reservoir for mitochondria, the cellular engines responsible for Adenosine Triphosphate (ATP) production. Metabolic disease and the physiological process of aging are both characterized by a distinct "transcriptional signature" of mitochondrial impairment and reduced oxidative capacity.18 The loss of muscle tissue results in a net decrease in mitochondrial density, which can lead to a drop in the basal metabolic rate (BMR). If the BMR declines significantly, the patient faces an increased likelihood of weight regain—the "rebound effect"—once the pharmacological intervention is ceased or the dose is plateaued.1
Physiological Adaptive Responses vs. Maladaptive Loss
It is essential to distinguish between adaptive and maladaptive lean mass loss. Some research suggests that a portion of the reduction in lean mass may be a physiological adjustment to a smaller body size, as a lighter individual requires less structural muscle to support and move their weight.1 Studies using magnetic resonance imaging (MRI) and skeletal muscle volume z-scores indicate that in certain populations, the reduction in muscle volume is commensurate with the overall weight reduction achieved.3 Furthermore, GLP-1 RAs have been shown to reduce myosteatosis—the infiltration of fat within skeletal muscle fibers—which can improve the "quality" and metabolic flexibility of the remaining muscle tissue.3
However, for vulnerable populations such as older adults, the frail, or those with pre-existing sarcopenia, even a proportional loss of muscle can have devastating functional consequences. Sarcopenic obesity—the presence of excess fat alongside critically low muscle mass—increases the risk of physical disability and cardiometabolic decline.1 Therefore, the preservation of muscle mass must be viewed not as an optional aesthetic goal, but as a metabolic priority during GLP-1 therapy. Resistance training has been uniquely identified as a strategy capable of reversing the transcriptional signature of aging in human skeletal muscle.18 By engaging in structured mechanical loading, older and metabolically compromised adults can rejuvenate mitochondrial function to levels approximating a younger physiological age, thereby offsetting the catabolic risks of their medication.18
The Minimum Effective Dose (MED) Framework
To address the metabolic challenges of GLP-1 therapy while ensuring patient adherence, this framework adopts the "Minimum Effective Dose" (MED) philosophy. This approach seeks to provide the smallest mechanical stimulus necessary to trigger systemic hormonal growth mechanisms without overtaxing the patient’s limited recovery resources.23 This is particularly relevant for individuals on GLP-1 therapy who may experience chronic fatigue, nausea, or decreased energy availability due to their caloric deficit.
Mechanics of Cadence and Muscular Intensity
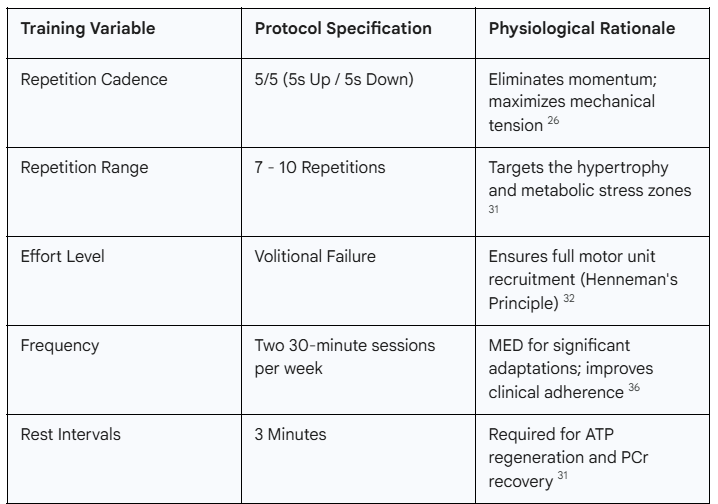
The protocol centers on a "Super Slow" cadence, typically utilizing a 5-second concentric phase followed by a 5-second eccentric phase (5/5). The primary physiological rationale for this tempo is the elimination of momentum. In traditional resistance training, the use of explosive concentric movements allows for a "launching" of the weight, where the initial acceleration carries the load through the sticking point, reducing the mechanical tension on the muscle for a significant portion of the range of motion.26 By slowing the movement, the muscle is forced to maintain constant mechanical tension throughout the entire lift, maximizing the metabolic stress on the fibers.26
Intensity is defined in this framework by the achievement of volitional muscular failure. According to Henneman’s Size Principle, motor units are recruited in an orderly fashion from smallest to largest. Low-threshold, slow-twitch (Type I) fibers are recruited first, followed by intermediate (Type IIa) and eventually high-threshold, fast-twitch (Type IIx) fibers as the effort becomes more demanding.31 Training to momentary failure—the point at which a further repetition is impossible despite maximal effort—ensures that the highest-threshold fast-twitch motor units are recruited and fatigued.26 These Type II fibers have the greatest potential for hypertrophy and play a crucial role in maintaining explosive strength and metabolic health.30
While some studies have shown that traditional speed reps may produce greater improvements in peak power and total energy expenditure compared to super slow training, the super slow method is uniquely advantageous for clinical populations due to its superior safety profile.29 By avoiding the high peak forces associated with acceleration and deceleration, the risk of acute musculoskeletal injury is significantly mitigated, making it an ideal choice for patients who are overweight or have underlying joint pathologies.26
Frequency, Duration, and the Molecular Clock
A critical component of the MED framework is its time efficiency. Clinical research suggests that effective hypertrophic signaling can be achieved with a remarkably low total volume. Meta-regressions of resistance training dosage indicate that performing as few as 1 to 5 sets per muscle group per week can still produce meaningful increases in strength and size.23 For the patient on GLP-1 therapy, a commitment of approximately four hours per month—divided into two 30-minute sessions per week—is sufficient to provide the stimulus required to preserve LBM.36
Consistency is further enhanced by aligning these sessions with the body’s circadian rhythms. Skeletal muscle contains an endogenous molecular clock, governed by a transcriptional-translational feedback loop involving genes such as Bmal1 and its repressor, Chrono.41 These muscle-specific rhythms regulate 24-hour cycles of glucose metabolism, insulin sensitivity, and autophagy.41 Engaging in strategic morning workouts can help reinforce these rhythms, potentially enhancing the muscle's metabolic flexibility and improving its capacity for glucose disposal.41
Structural Integrity and the 12-Week Conditioning Phase
A common error in the clinical management of exercise in patients with obesity is the failure to account for the differential adaptation rates of various musculoskeletal tissues. While muscle tissue is highly vascular and adapts rapidly to the stimulus of resistance training—often showing neural strength gains within 2 to 4 weeks and morphological changes within 6 to 8 weeks—tendons and ligaments have a significantly more limited blood supply and a slower rate of metabolic turnover.42
The Physiology of Tendon Adaptation
Research indicates that tendons require a much longer duration of mechanical loading to achieve meaningful increases in stiffness and cross-sectional area. Meta-analyses of training studies demonstrate that while some stiffness increases can be detected within 8 weeks, consistent and robust adaptations generally require 12 or more weeks of sustained loading.42 During this period, tendons undergo material property modifications, including increased collagen cross-linking and improved fiber organization.42
This adaptation gap creates a period of vulnerability. When a patient begins an aggressive resistance training program, their muscle strength often increases faster than their tendons can adjust. This "muscle-tendon imbalance" means the strengthened muscles can generate forces that exceed the structural tolerance of the unconditioned tendons, leading to an elevated risk of rupture or chronic tendinopathy.42
Metabolic Syndromes and Increased Injury Risk
The risk of connective tissue injury is further compounded by the metabolic status of the GLP-1 patient. Obesity and diabetes are systemic determinants of tendon pathology. Individuals with metabolic syndrome have approximately 2.5 times higher risk of tendon injury, and those with chronic hyperglycemia (HbA1c > 5.7%, even in the prediabetic range) have a 3 times higher risk of lower extremity tendon injury.46

Chronic hyperglycemia leads to the accumulation of advanced glycation end-products (AGEs) within the collagen-rich matrix of the tendon. These AGEs form covalent cross-links between collagen fibers, altering the tissue’s mechanical properties and making it more brittle and prone to microruptures.46 Additionally, the systemic state of low-grade inflammation associated with obesity releases pro-inflammatory cytokines, such as TNF-a and PG E2, which further disrupt tendon homeostasis and impair the healing response.44
The "Hardening the Chassis" Protocol
To prevent these injuries, a mandatory 12-week conditioning phase is required to "harden the chassis" of the patient. This phase systematically prepares the connective tissues for the high mechanical loads of the subsequent hypertrophy-focused MED protocol.
Weeks 1–4: Focus on Neuromuscular Learning. Training loads are kept low (50–60% of capacity) to prioritize the perfection of movement patterns and increase the lubrication of the synovial joints.37 This period allows the brain to learn "reciprocal inhibition"—the ability to turn off opposing muscles during a lift—which enhances movement efficiency and reduces initial injury risk.42
Weeks 5–8: Initiation of Collagen Turnover. Loads are gradually increased to initiate material property changes in the tendons. Research shows that sustained contractions (e.g., the 5/5 cadence) are more effective at increasing tendon stiffness than explosive or plyometric loading.42
Weeks 9–12: Structural Development. This period bridges the gap to performance-based hypertrophy. By the end of this phase, the material stiffness of the tendons and the strength of the muscles should be more closely aligned, allowing for safer progression into higher-intensity training.42
Kinetic Protocol: Superset Architecture
The resistance routine utilizes a superset architecture to maximize metabolic stress and improve time efficiency. A superset consists of two exercises performed back-to-back with no rest, targeting either opposing muscle groups or different movement planes.25 This structure is particularly effective for glycogen depletion—a key goal for patients with insulin resistance.6
Supersets for Metabolic Recovery and Efficiency
The routine is divided into four primary exercise groups. Each group is performed for two rounds, with a 3-minute rest period between sets and rounds. This rest interval is essential for the regeneration of the Phosphocreatine (PCr) system and the clearance of metabolites, ensuring that the high intensity required for volitional failure can be maintained in the subsequent round.25
Superset 1: Bench Press (Horizontal Press) and Lunges (Unilateral Leg). This pairing provides a strong systemic stimulus by engaging the largest muscle groups of the chest, shoulders, and legs. The unilateral nature of the lunge improves balance and core stability, which are often reduced in individuals with significant weight-related mobility issues.20
Superset 2: Overhead Military Press (Vertical Press) and Leg Press (Bilateral Leg). This group targets vertical pressing strength and allows for heavy loading of the lower body in a stable, machine-based environment, which is often safer for the beginner or obese patient than a free-weight squat.25
Superset 3: Seated Rows (Horizontal Pull) and Leg Curls (Posterior Chain). This pairing focuses on the pulling muscles of the back and the critical but often neglected hamstring group. Strengthening the posterior chain is essential for protecting the lower back and improving gait efficiency.25
Superset 4: Lat Pull Downs (Vertical Pull) and Leg Extensions (Anterior Isolation). This final group serves as a metabolic finish. The isolation of the quadriceps in the leg extension allows for maximal glycogen depletion in a muscle group that is a primary determinant of systemic glucose disposal.6
The use of resistance machines is generally recommended over free weights for this population. Machines provide a lower risk of injury by guiding the movement through a fixed path, allowing the patient to focus entirely on the intensity of the muscular contraction and the slow cadence rather than the coordination and balance required for free-weights.26
Nutritional Precision and Anabolic Resistance
For individuals on GLP-1 therapy, the challenge of muscle preservation is compounded by "anabolic resistance." This condition, prevalent in aging and calorie-restricted populations, occurs when the muscle cells become less responsive to the anabolic signals of protein and exercise.52 Overcoming this resistance requires a precise bolus of protein that meets a specific "Leucine threshold."
The Leucine Threshold and mTOR Pathway
Leucine is a unique branched-chain amino acid (BCAA) that serves as the primary molecular signal to activate the mammalian target of rapamycin (mTOR) pathway, the central switch for muscle protein synthesis (MPS).35 Research indicates that elevating plasma leucinemia is a potent stimulator of MPS, but there is a "muscle full" state where additional amino acids provide no further benefit.53
To maximize MPS in older or energy-restricted adults, a bolus of approximately 40 grams of high-quality protein is recommended per meal. This dose is necessary to ensure that the Leucine threshold—typically around 3.5 to 4.2 grams—is reached.35 For instance, enriching a protein drink with 4.2 grams of leucine has been shown to significantly augment the anabolic response following resistance exercise compared to protein alone.54 For the GLP-1 patient, who may struggle to consume large volumes of food, utilizing high-quality, rapidly-digested protein sources (such as whey or specific amino acid supplements) is an effective strategy to reach this threshold without overtaxing their appetite-suppressed gastric system.9
Creatine Hydrochloride (HCl) for Gastrointestinal Comfort
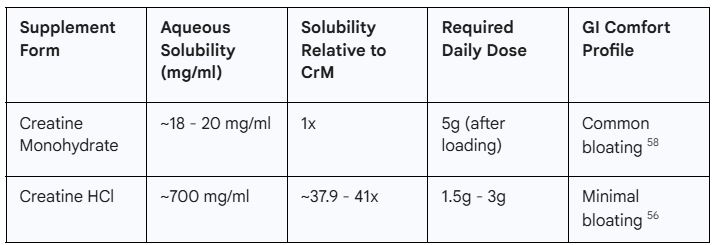
Creatine is one of the most effective and safe ergogenic aids for enhancing strength and preserving LBM.56 While Creatine Monohydrate (CrM) is the most widely researched form, Creatine Hydrochloride (Cr-HCl) is often preferred for patients on GLP-1 therapy due to its superior solubility and GI profile.57
Cr-HCl is molecularly bound with hydrochloric acid, a modification that reportedly makes it 37.9 to 41 times more soluble in water than CrM at 25°C.56 This higher solubility has significant clinical implications:
Bioavailability: Greater solubility and permeability in the intestinal tract allow for better absorption, potentially requiring smaller doses to achieve muscle saturation.56
Reduced Side Effects: Standard CrM loading often causes bloating, water retention, and gastrointestinal discomfort—side effects that are particularly problematic for patients already dealing with GLP-1-induced nausea or delayed gastric emptying.9
Dosing: Because of its enhanced bioavailability, Cr-HCl is effective at lower doses (1.5–3g daily) and does not typically require the high-dose loading phase associated with CrM.58
While some studies have shown that CrM remains the most cost-effective option and provides similar long-term strength gains, for the specific sub-population of GLP-1 patients, the reduction in GI distress associated with Cr-HCl makes it a clinically superior recommendation.56
Chronobiology and Gender-Specific Nutrient Timing
Clinical outcomes in metabolic preservation are significantly influenced by gender-specific physiological responses. Research from Dr. Stacy Sims emphasizes that "women are not small men," and that female hormonal architecture—particularly the sensitivity to energy availability and cortisol—requires distinct nutrient timing strategies.61
The Cortisol-Catabolic Trap in Women
For women, especially those in perimenopause or menopause, exercising in a fasted state can be profoundly detrimental. Cortisol levels naturally peak approximately 30 minutes after waking.61 For a female patient on GLP-1 therapy, combining this natural cortisol peak with a fasted state and the mechanical stress of exercise can trigger a high sympathetic drive and a state of "low energy availability" (LEA).61 In this state, the body prioritizes the breakdown of muscle tissue to provide glucose for the brain and the workout, while simultaneously down-regulating other key hormones like thyroid hormone and estrogen.61
This leads to a "catabolic trap" where the female patient may feel "tired but wired" and experience stalled weight loss, particularly around the abdominal region, due to the chronically elevated cortisol.61 To blunt this response, Dr. Sims recommends that female patients consume a small bolus of protein (15–40g) and potentially some easy-to-digest carbohydrates 30–45 minutes pre-workout.61 This protein bolus provides the necessary amino acid substrate to signal to the brain that the body is in an anabolic state, thereby protecting muscle mass and improving recovery.62
Post-Workout Refueling Windows
The "anabolic window" also differs by gender. Men typically maintain an elevated metabolic rate and a longer window for glycogen resynthesis (up to 3 hours post-exercise), giving them more flexibility in timing their post-workout meals.62 However, women’s metabolisms return to baseline much faster—often within 60 to 90 minutes.61 Consequently, it is critical for female patients to consume high-quality protein (at least 35g) within 30 to 45 minutes of finishing their training session to initiate muscle repair and stop the catabolic process.61
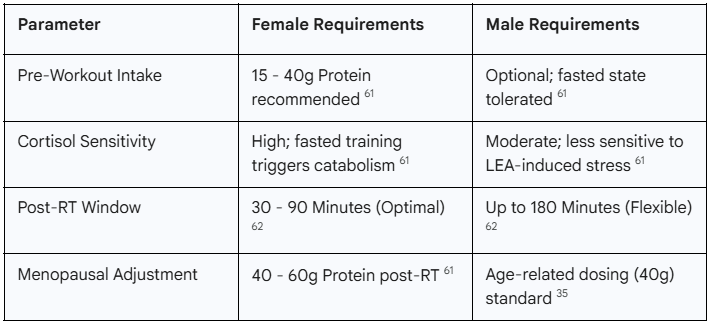
In perimenopause and menopause, these requirements are even more stringent. As estrogen—which is anti-inflammatory and muscle-sparing—declines, women must rely more heavily on external protein signals and heavy mechanical loads to maintain bone and muscle integrity.64
Integrating the "Molecular Rejuvenation" of Muscle
One of the most profound insights for patients on GLP-1 therapy is the ability of resistance training to reverse biological aging at the cellular level. Skeletal muscle from older adults typically displays a transcriptional signature of mitochondrial impairment, where genes involved in energy metabolism are significantly down-regulated.18
Melov and colleagues (2007) evaluated the effect of six months of resistance exercise on these profiles. They identified 596 genes that were differentially expressed with age, particularly "Cluster 2" genes, which showed a 39-fold enrichment in genes directly related to mitochondrial metabolism and electron transport.19 Following the training program, the transcriptional signature of these aging individuals was "markedly reversed" back toward youthful levels.18 Specifically, 179 of the 596 age-associated genes showed a statistically significant reversal, meaning that both up-regulated and down-regulated aging genes shifted back toward the expression levels found in young adults.18
This molecular rejuvenation has direct implications for the "metabolic rate depression" often seen during rapid weight loss. By improving mitochondrial density and oxidative capacity through resistance training, the patient can theoretically maintain a higher resting metabolic rate, making long-term weight maintenance more achievable.1
Metabolic Flexibility and Myosteatosis
While the absolute loss of lean mass is a primary concern, the "quality" of the muscle that remains must also be analyzed. Obesity is characterized by myosteatosis, the infiltration of both intermuscular fat (between muscle fibers) and intramyocellular fat (within the myocytes).22 This ectopic fat storage is a major driver of insulin resistance, as it interferes with normal insulin signaling pathways (e.g., PI3K/Akt signaling) and triggers the release of inflammatory cytokines.8
GLP-1 RAs have been shown to be particularly effective at reducing this intramuscular lipid accumulation. Studies using MRI have demonstrated that semaglutide treatment can significantly lower the skeletal muscle steatosis fraction over six months, even when total muscle volume modestly declines.17 This reduction in "fatty muscle" improves the muscle’s metabolic flexibility—its ability to efficiently switch between burning carbohydrates and fats.3 Clinically, this is reflected in improved functional scores (such as the 6-minute walk test and chair-rise time) and unchanged handgrip strength, despite the measured volumetric loss of LBM.1 Therefore, the goal of the clinician should be to maximize this "adaptive" loss of fat while minimizing the "maladaptive" loss of actual contractile protein.3
Conclusion: A Multi-Modal Clinical Imperative
The catabolic risk of GLP-1 therapy represents a significant challenge to the long-term success of weight management programs. For the patient, muscle preservation is not a secondary aesthetic goal but a metabolic necessity that determines the sustainability of their health outcomes beyond the duration of pharmacological treatment. This research report provides an integrated framework designed to protect the patient from the potential pitfalls of rapid weight loss.
The Minimum Effective Dose (MED) resistance training protocol offers a time-efficient solution that recruits the full range of motor units while minimizing systemic inflammation and injury risk. By utilizing a "Super Slow" cadence of 5/5 to failure, patients can achieve significant neuromuscular adaptations with as little as four hours of total monthly training. This mechanical stimulus is essential for reversing the transcriptional signature of aging and maintaining mitochondrial integrity.
Crucially, the implementation of a 12-week conditioning phase respects the slower adaptation rates of connective tissues, particularly in the context of the elevated injury risk associated with metabolic syndrome and hyperglycemia. When this physical stimulus is paired with a precision nutritional strategy—specifically, a 40g bolus of leucine-rich protein and the strategic use of Creatine HCl—the patient can overcome anabolic resistance and ensure that weight loss is primarily adipose-derived.
Finally, the integration of gender-specific chronobiology, as championed by Dr. Stacy Sims, ensures that female patients are protected from the catabolic traps of elevated cortisol and low energy availability. By providing protein pre-workout and refueling within a tight post-workout window, the female metabolic profile can remain anabolic despite the rigors of GLP-1 therapy. By following this multi-modal approach, clinicians can ensure that the "revolution" in obesity management is defined by a true improvement in body composition and long-term functional longevity, rather than a mere reduction in the numbers on a scale.
Works cited
Muscle Mass and Glucagon-Like Peptide-1 Receptor Agonists ..., accessed February 8, 2026, https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.124.067676?doi=10.1161/CIRCULATIONAHA.124.067676
Effects of liraglutide on body composition in people living with obesity or overweight: A systematic review | Request PDF - ResearchGate, accessed February 8, 2026, https://www.researchgate.net/publication/388655132_Effects_of_liraglutide_on_body_composition_in_people_living_with_obesity_or_overweight_A_systematic_review
Muscle Mass and Glucagon-Like Peptide-1 Receptor Agonists: Adaptive or Maladaptive Response to Weight Loss? - American Heart Association Journals, accessed February 8, 2026, https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.124.067676
Semaglutide Usage as a Weight Loss Management - Literature ..., accessed February 8, 2026, https://biomedres.us/pdfs/BJSTR.MS.ID.009179.pdf
Semaglutide Usage as a Weight Loss Management - Literature Review, accessed February 8, 2026, https://biomedres.us/fulltexts/BJSTR.MS.ID.009179.php
GLUT4: a key player regulating glucose homeostasis? Insights from transgenic and knockout mice - Taylor & Francis, accessed February 8, 2026, https://www.tandfonline.com/doi/pdf/10.1080/09687680110072131
Role of Skeletal Muscle in Insulin Resistance and Glucose Uptake - PMC - NIH, accessed February 8, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC8074531/
Metabolic and molecular regulation in skeletal muscle dysfunction and regeneration, accessed February 8, 2026, https://www.frontiersin.org/journals/cell-and-developmental-biology/articles/10.3389/fcell.2025.1651553/full
(PDF) "Semaglutide Usage as a Weight Loss Management - Literature Review", accessed February 8, 2026, https://www.researchgate.net/publication/384386818_Semaglutide_Usage_as_a_Weight_Loss_Management_-_Literature_Review
Impact of Semaglutide on Body Composition in Adults With Overweight or Obesity: Exploratory Analysis of the STEP 1 Study - PMC, accessed February 8, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC8089287/
Ozempic Muscle Loss: How to Prevent Lean Mass Reduction | BodySpec, accessed February 8, 2026, https://www.bodyspec.com/blog/post/ozempic_muscle_loss_how_to_prevent_lean_mass_reduction
Lean mass loss on GLP-1 receptor agonists: a downside of the “miracle drugs” - Peter Attia, accessed February 8, 2026, https://peterattiamd.com/the-downside-of-glp-1-receptor-agonists/
accessed February 8, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC12536186/#:~:text=In%20the%20SURMOUNT%2D1%20trial%2C%20124%20participants%20treated%20with%20tirzepatide,of%20weight%20loss%20as%20LST.
Body composition changes during weight reduction with tirzepatide in the SURMOUNT-1 study of adults with obesity or overweight - PubMed, accessed February 8, 2026, https://pubmed.ncbi.nlm.nih.gov/39996356/
Does Tirzepatide Cause Muscle Loss? What the SURMOUNT-1 Study Reveals, accessed February 8, 2026, https://openhouseclinic.com/en/insights/mounjaro_lossfatormuscle_en/
Send in the signals : studies on the mechanisms of insulin resistance in human skeletal muscle - Helda - University of Helsinki, accessed February 8, 2026, https://helda.helsinki.fi/items/5c59d8a5-ed0d-4b0f-ac5f-05c8704df1bc
Impact of Incretin-Based Therapy on Skeletal Muscle Health - PMC - NIH, accessed February 8, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC12471476/
Resistance Exercise Reverses Aging in Human Skeletal Muscle - ResearchGate, accessed February 8, 2026, https://www.researchgate.net/publication/6312760_Resistance_Exercise_Reverses_Aging_in_Human_Skeletal_Muscle
Resistance Exercise Reverses Aging in Human Skeletal Muscle ..., accessed February 8, 2026, https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0000465
JON to ONE - Evidence - STRENGTH4HEALTH, accessed February 8, 2026, https://www.strength4health.co.uk/evidence/
Resistance exercise reverses aging in human skeletal muscle - PubMed - NIH, accessed February 8, 2026, https://pubmed.ncbi.nlm.nih.gov/17520024/
Epidemiology of Myosteatosis - PMC - PubMed Central - NIH, accessed February 8, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC2872135/
The Minimum Effective Training Dose Required for 1RM Strength in Powerlifters - PMC, accessed February 8, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC8435792/
Train Smarter, Not Longer: The Minimum Effective Dose for Muscular Development - Patroklos "Pak" Androulakis Korakakis - Google Books, accessed February 8, 2026, https://books.google.com/books/about/Train_Smarter_Not_Longer.html?id=q6y2EQAAQBAJ
Minimum Effective Dose Exercise - Will Campbell Fitness, accessed February 8, 2026, https://www.willcampbellfitness.com/blog/minimum-effective-dose-for-exercise
Evidence based resistance training recommendations Fisher, James - Southampton Solent University, accessed February 8, 2026, https://pure.solent.ac.uk/ws/files/10205168/ms_2011_03_08_Fisher.pdf
Repetition Speed Recommendations - Drew Baye, accessed February 8, 2026, https://baye.com/repetition-speed-recommendations/
Bodyweight HIT Workouts - Drew Baye, accessed February 8, 2026, https://baye.com/bodyweight-hit-workouts/
Are Jay Vincent's claims legitimate (High Intensity Training advocate/fitness industry skeptic)? : r/AdvancedFitness - Reddit, accessed February 8, 2026, https://www.reddit.com/r/AdvancedFitness/comments/sra6yd/are_jay_vincents_claims_legitimate_high_intensity/
Equalization of Training Protocols by Time Under Tension Determines the Magnitude of Changes in Strength and Muscular Hypertrophy | Request PDF - ResearchGate, accessed February 8, 2026, https://www.researchgate.net/publication/350472028_Equalization_of_Training_Protocols_by_Time_Under_Tension_Determines_the_Magnitude_of_Changes_in_Strength_and_Muscular_Hypertrophy
Rep Range For Hypertrophy | Jim Stoppani, accessed February 8, 2026, https://www.jimstoppani.com/training/rep-range/
Manipulating Resistance Training Variables to Induce Muscle Strength and Hypertrophy: A Brief Narrative Review - ResearchGate, accessed February 8, 2026, https://www.researchgate.net/publication/362002340_Manipulating_Resistance_Training_Variables_to_Induce_Muscle_Strength_and_Hypertrophy_A_Brief_Narrative_Review
Evidence-Based Resistance Training Recommendations - FitGreyStrong, accessed February 8, 2026, https://fitgreystrong.com/wp-content/uploads/2019/11/Evidence-Based_Resistance_Training_Recommendations.pdf
Corporate Warrior | PDF | Tort | Strength Training - Scribd, accessed February 8, 2026, https://www.scribd.com/document/425204989/Corporate-Warrior
(PDF) Amino Acids and Implications for Athletes (protein synthesis and recovery), accessed February 8, 2026, https://www.researchgate.net/publication/262867337_Amino_Acids_and_Implications_for_Athletes_protein_synthesis_and_recovery
Journal of Novel Physiotherapies - Effects of Whole-Body EMS on Post-ACL Reconstruction General Conditioning - A Retrospective Comparative Study - OMICS International, accessed February 8, 2026, https://www.omicsonline.org/open-access/effects-of-wholebody-ems-on-postacl-reconstruction-general-conditioning--a-retrospective-comparative-study-114921.html
Progression Models in Resistance Training for Healthy Adults - tourniquets.org, accessed February 8, 2026, https://tourniquets.org/wp-content/uploads/PDFs/ACSM-Progression-models-in-resistance-training-for-healthy-adults-2009.pdf
Effect of Explosive versus Slow Contractions and Exercise Intensity on Energy Expenditure | Request PDF - ResearchGate, accessed February 8, 2026, https://www.researchgate.net/publication/6078664_Effect_of_Explosive_versus_Slow_Contractions_and_Exercise_Intensity_on_Energy_Expenditure
(PDF) The Resistance Training Dose-Response: Meta-Regressions Exploring the Effects of Weekly Volume and Frequency on Muscle Hypertrophy and Strength Gain - ResearchGate, accessed February 8, 2026, https://www.researchgate.net/publication/384628335_The_Resistance_Training_Dose-Response_Meta-Regressions_Exploring_the_Effects_of_Weekly_Volume_and_Frequency_on_Muscle_Hypertrophy_and_Strength_Gain
AEROSPACE MEDICINE AND BIOLOGY - NASA Technical Reports Server, accessed February 8, 2026, https://ntrs.nasa.gov/api/citations/19710021380/downloads/19710021380.pdf
Skeletal-Muscle-Specific Overexpression of Chrono Leads to Disruption of Glucose Metabolism and Exercise Capacity - MDPI, accessed February 8, 2026, https://www.mdpi.com/2075-1729/12/8/1233
The Throwing Timeline: Baseball Strength is Not Instant - Oates Specialties, accessed February 8, 2026, https://oatesspecialties.com/blogs/default-blog/the-science-of-tissue-adaptation-why-your-arm-needs-time-to-get-strong
TIME COURSE OF CHANGES IN MUSCLE AND TENDON PROPERTIES DURING STRENGTH TRAINING AND DETRAINING - Paulo Gentil, accessed February 8, 2026, https://paulogentil.com/pdf/Time%20Course%20of%20Changes%20in%20Muscle%20and%20Tendon%20Properties%20During%20Strength%20Training%20and%20Detraining.pdf
Lower calf raise efficiency in obesity is partially related to higher triceps surae MTU passive stiffness, hysteresis, and reduced relative strength, accessed February 8, 2026, https://journals.physiology.org/doi/full/10.1152/japplphysiol.00702.2024?doi=10.1152/japplphysiol.00702.2024
Response of tibialis anterior tendon to a chronic exposure of stretch-shortening cycles: age effects - PubMed Central, accessed February 8, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC2710328/
(PDF) Chronic hyperglycemia, hypercholesterolemia and metabolic ..., accessed February 8, 2026, https://www.researchgate.net/publication/351438896_Chronic_hyperglycemia_hypercholesterolemia_and_metabolic_syndrome_are_associated_with_risk_of_tendon_injury
Effect of Diabetes on Tendon Structure and Function: Not Limited to Collagen Crosslinking, accessed February 8, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC9846394/
Obesity Increases the Risk of Tendinopathy, Tendon Tear and Rupture, and Postoperative Complications: A Systematic Review of Clinical Studies - PMC, accessed February 8, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC7371074/
How obesity modifies tendons (implications for athletic activities) - PMC - PubMed Central, accessed February 8, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC4241419/
(PDF) Progression models in resistance training for healthy adults [ACSM position stand], accessed February 8, 2026, https://www.researchgate.net/publication/235653976_Progression_models_in_resistance_training_for_healthy_adults_ACSM_position_stand
Effects of high-intensity swimming training on GLUT-4 and glucose transport activity in rat skeletal muscle - American Physiological Society Journal, accessed February 8, 2026, https://journals.physiology.org/doi/10.1152/jappl.2001.90.6.2019
Biochemical Pathways of Sarcopenia and Their Modulation by Physical Exercise: A Narrative Review - PMC, accessed February 8, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC5632757/
Targeted Leucine Supplementation and Dietary Protein Distribution Strategies: Applications for Recovery from Exercise in Trained, accessed February 8, 2026, https://doras.dcu.ie/22625/1/Michelle%20Hone%20Thesis%20FINAL.pdf
Enriching a protein drink with leucine augments muscle protein synthesis after resistance exercise in young and older men | Request PDF - ResearchGate, accessed February 8, 2026, https://www.researchgate.net/publication/301773264_Enriching_a_protein_drink_with_leucine_augments_muscle_protein_synthesis_after_resistance_exercise_in_young_and_older_men
Plasma concentrations of selected AAs: phenylalanine (A), leucine (B),... - ResearchGate, accessed February 8, 2026, https://www.researchgate.net/figure/Plasma-concentrations-of-selected-AAs-phenylalanine-A-leucine-B-and-threonine-C_fig1_225056132
Supplementing With Which Form of Creatine (Hydrochloride or ..., accessed February 8, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC11629957/
Best Form of Creatine: The Simple, Proven Truth - Liv Hospital, accessed February 8, 2026, https://int.livhospital.com/best-form-of-creatine-truth/
Creatine HCl and Creatine Monohydrate Improve Strength but Only Creatine HCl Induced Changes on Body Composition in Recreational Weightlifters - Scientific Research Publishing, accessed February 8, 2026, https://www.scirp.org/journal/paperinformation?paperid=62283
Creatine HCL vs. Monohydrate | Which Is Better? - MYPROTEIN™, accessed February 8, 2026, https://ca.myprotein.com/blog/supplements/creatine-hcl-vs-monohydrate-better/
Creatine HCl and Creatine Monohydrate Improve Strength but Only Creatine HCl Induced Changes on Body Composition in Recreational Weightlifters - ResearchGate, accessed February 8, 2026, https://www.researchgate.net/publication/288670717_Creatine_HCl_and_Creatine_Monohydrate_Improve_Strength_but_Only_Creatine_HCl_Induced_Changes_on_Body_Composition_in_Recreational_Weightlifters
Dr. Stacy Sims: Female-Specific Exercise & Nutrition for Health, Performance & Longevity, accessed February 8, 2026, https://www.getrecall.ai/summary/fitness/dr-stacy-sims-female-specific-exercise-and-nutrition-for-health-performance-and-longevity
Why Women Need a Different Approach to Post-Training Nutrition and Fasting, accessed February 8, 2026, https://www.avosstrength.com/blog/2025/2/10/why-women-need-a-different-approach-to-post-training-nutrition-and-fasting
Why Women Need to Fuel Differently Around Workouts - The Studio Salcombe, accessed February 8, 2026, https://thestudiosalcombe.com/why-women-need-to-fuel-differently-around-workouts/
The Truth About Fasting for Women | Dr. Stacy Sims & Dr. Andrew Huberman - YouTube, accessed February 8, 2026, https://www.youtube.com/watch?v=NX5WvmzfDck
The relationship between Nutrition, Exercise and Female Hormones, accessed February 8, 2026, https://www.nutrition4change.com/articles/the-relationship-between-nutrition-exercise-and-female-hormones/
Effects of Tirzepatide on Skeletal Muscle Mass in Adults: A Systematic Review - PMC, accessed February 8, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC12394919/
Palmitate and oleate exert differential effects on insulin signalling and glucose uptake in human skeletal muscle cells - PMC - PubMed Central, accessed February 8, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC5510447/